
Winning a grant should feel like relief. Yet it often lands like a stress test.
Think of your organization like a body after bariatric surgery. Just as patients need a stomach pouch reset to recalibrate their eating limits and avoid overload, a grant win calls for an intake capacity reset, a focused recalibration of your referral handling to match surging demands.
More money usually means more referrals, more outreach, more reporting, and more eyes on your performance. If your intake process was already tight, a grant win can push it past the breaking point. This reset helps you absorb the opportunity without burning out your team.
The first 90 days matter because they mark the critical stage in your organization’s efficiency journey, setting the pace, rules, and ownership your growth will follow.
Key takeaways
- A grant win does not fix intake strain by itself. It often exposes weak triage, unclear ownership, and hidden backlog, like a clogged intake causing an engine to stall under the increased load of new funding.
- Your first move is not new software. Your first move is a clear picture of volume, handoffs, and decision rights.
- Failing to adjust is like weight regain for an organization that just slimmed down its processes. In 90 days, you can stabilize intake if you simplify entry points, tighten routing, and track a small set of measures.
A grant win can overload a shaky intake system fast
A new grant increases pressure in two directions at once. You need to serve more people, and you need to prove results sooner.
That sounds manageable on paper. In practice, intake is where the strain shows up first, much like the transformative impact of a gastric sleeve or gastric bypass where capacity is suddenly limited but demands are high. Calls pile up. Forms sit unread. Staff create side spreadsheets clogged with carbon deposits of administrative gunk. Meanwhile, partners keep sending referrals because the funding announcement raised expectations, leading to stomach stretching if you take on too much too fast.
This is a capacity absorption problem, not a motivation problem, akin to a throttle body choked by buildup in referral side-channels. If you want a useful outside view of that issue, Firefly Giving’s piece on nonprofit capacity absorption explains why new funding can outpace an organization’s ability to take it in well. Similarly, OpenGrants’ guide to capacity-building grants is a good reminder that infrastructure work is part of impact, not a distraction from it.
The warning signs are usually easy to spot:
- Intake arrives through too many doors.
- Staff don’t share the same triage rules.
- Referrals get sent, but outcomes stay unknown.
- Reporting depends on cleanup at the end of the month.
When you see those patterns, don’t treat them as minor admin issues. They affect fairness, staff load, client experience, and funder trust.
If you need a quick way to size the problem, use an intake-to-outcome clarity checklist. It helps you see where requests slow down, where handoffs fail, and which risks deserve attention first.
Start with the intake system you actually have
Most teams describe the process they meant to build. Your reset depends on the process people use today, which runs like an electronic control unit managing your organization’s metabolic rate.
Begin by mapping every intake path. Include phone, email, web forms, walk-ins, partner referrals, and staff side channels. Then mark three things: who reviews each request, how priority gets set, and what counts as a completed handoff.
You are looking for drag, not perfection. Where does work wait, like engine idle speed dropping without new fuel (referrals) injected? Where does ownership blur? Where do staff re-enter the same details, overworking the idle air control valve that maintains baseline operations? Those spots usually cost more than the obvious backlog.
Keep this part plain. You do not need a long study. You need one page that leadership can trust. That page should show weekly volume, average response time, top routing reasons, and the points where clients disappear.
Then assign one accountable owner for intake operations during the reset. That person does not need to do every task. They do need authority to make routing calls, surface bottlenecks, and force decisions when the queue slips.
If requests come in from everywhere, reduce the noise early. A single front door intake design guide can help you narrow channels and set shared rules. That step alone often buys back more capacity than a rushed tool purchase.
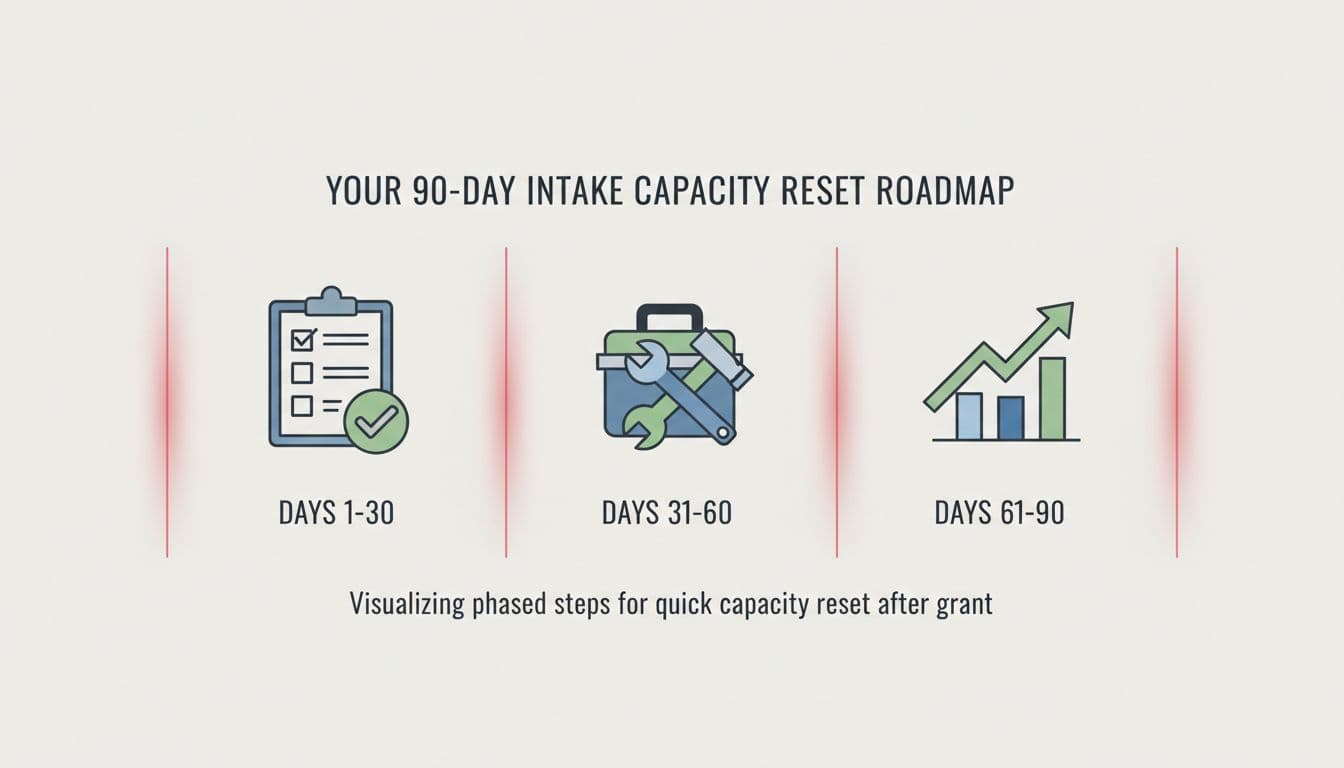
Your 90-day intake capacity reset roadmap
You do not need to rebuild everything in one quarter. You do need clear moves in the right order.
Think of this structured approach as a post-op diet for the organization, similar to a five day pouch reset but scaled for business operations. It guides your intake system through recovery phases, starting simple and building sustainably.
This simple view keeps the first 90 days grounded.
| Window | Main goal | What you do |
|---|---|---|
| Days 1-30 | See reality | Map all entry points, count weekly volume, name one intake owner, define urgent vs routine |
| Days 31-60 | Reduce drag | Close duplicate channels, tighten triage rules, set response targets, remove duplicate data entry |
| Days 61-90 | Build control | Add simple dashboards, review aging work weekly, fix referral follow-up, document the new process |
In the first month, resist the urge to launch a new platform. If your routing logic is fuzzy, software will only speed up confusion. Treat this phase like a liquid diet, where only essential information flows to assess reality without overwhelming the system.
By days 31 through 60, your job is to make the process lighter, much like introducing pureed foods and soft foods as the system begins to handle more complexity. That may mean fewer form fields, fewer exceptions, and firmer rules about who can bypass intake. Growth creates pressure for workarounds. Your reset should do the opposite.
By days 61 through 90, focus on staying power. Add a weekly review rhythm. Track only the measures that change decisions. For example, use time to first response, queue size by priority, percentage routed correctly on first review, and known referral outcomes.
If your work depends on outside partners, tighten the handoff. A closed-loop referral playbook helps you move from “we sent it” to “we know what happened.” That shift matters because grant-funded growth often increases partner volume before it improves partner coordination.
Protect reporting, trust, and staff capacity while you scale
A strong intake capacity reset is not only about speed. It is also about trust.
When demand rises, teams often borrow capacity from the wrong places. They skip notes. They widen access. They let definitions drift. This unstructured growth adds fat instead of building muscle mass through strength training. Later, reporting gets messy and leadership loses confidence in the numbers.
So, keep your reporting model simple and stable. Define what counts as intake, triage, accepted, referred, waitlisted, and closed. Use those terms the same way across programs. Otherwise, every board update turns into a debate about definitions. Treat consistent definitions as healthy habits for your calorie intake of funder resources and data.
Also protect your staff from heroics. If one high performer is holding the queue together through inbox rules and memory, your intake is fragile. A grant should reduce that fragility, not fund more of it. Efficient systems burn calories better, processing resources with the precision of smart protein consumption.
For a broader view of scaling without overloading your team, Grant Llama’s guide to nonprofit capacity and burnout is a useful reminder that growth without operating discipline is expensive.
FAQs about a 90-day intake capacity reset
Do you need new software to do this well?
Usually not in the first 90 days. First, fix intake paths, rules, ownership, and measures. Skip the protein shakes of quick-fix solutions that offer short-term boosts without building lasting system changes. Then you can judge whether your current tools are enough or whether a system change is worth the disruption.
Who should lead the reset?
Your best choice is usually an operations leader, like a bariatric surgeon performing the reset with precision and authority to make cross-team decisions. Intake touches program, data, reporting, and partner work, so the owner needs backing from senior leadership.
What if your grant requires quick expansion?
Move faster on scope control, not tool buying. Narrow channels, define priority rules, and limit exceptions. If you expand volume before you stabilize intake, your team will spend the grant period cleaning up a weight loss plateau of preventable chaos.
A grant win is good news, but it also reveals how much operational slack you really have. That is why the first 90 days should focus on managing stomach capacity through clearer visibility, stronger ownership, and a calmer intake rhythm.
If your team needs a sharper picture of where work slows down and why, a short technology clarity call can help you sort the signal from the noise.